Site of Care Optimization Offers Savings for Specialty Services
Summary
Across physician specialties, Medicare utilization and reimbursement data shows that site-of-care optimization can reduce expenditures for certain healthcare services.In the current environment of rising healthcare costs, ongoing reimbursement pressure, and continued physician employment and provider consolidation, providers must reconsider how to effectively and affordably offer care to patients. Services that may be provided across multiple sites of care (SOCs), such as procedures and imaging, offer a strong opportunity to increase efficiency, improve quality, and reduce cost when the SOC in which they are performed is optimized. Policies such as site-neutral payment can drive SOC choice and have been considered by Congress, various administrations, and private payers.
SOC optimization refers to the strategy of directing patients to the most cost-effective, clinically appropriate setting to receive a given healthcare service without sacrificing quality. Once clinical standards and technology allow a service to be safely rendered in a particular SOC, providers can encourage patients with the appropriate risk profile to seek–and payers can encourage providers to render–a given service in the lowest-cost SOC. This can reduce associated expenditures for both the patient and the payer while maintaining appropriate and sufficient reimbursement for the provider.
Lower-acuity SOCs like ambulatory surgery centers (ASCs) and physician offices can also offer an improved patient experience via more convenient access to care and an improved provider experience via dedicated operating room hours. For a procedure to be covered by Medicare in lower-acuity SOCs, it must not appear on Medicare’s Inpatient Only List (IPO). For a procedure to be covered by Medicare in the ASC setting, it must also be added to the ASC Covered Procedures List (CPL).
Specialty services constitute a key savings opportunity for several reasons. First, management by a dedicated class of specialty providers encourages the development of clear standards of care. Second, these services are often performed in a facility setting, such as a hospital outpatient department (HOPD) or ASC. Services performed in a facility setting incur a separate “facility fee” intended to cover expenses related to the facility itself (e.g., staffing, equipment, and overhead) in addition to the professional fee, which reimburses the physician for their time. In Medicare, the professional fee is the same across facility-based settings (i.e., HOPDs and ASCs), so the facility fee is responsible for the entire cost differential between these two settings, representing the savings opportunity.
Utilization Across Different Sites of Care
Underlying trends in utilization across SOCs inform the magnitude of savings that SOC optimization may generate, and different procedures and specialties have varying degrees of SOC optimization. For the Medicare population, Figure 1 shows the SOC breakdown for representative high-volume procedures in ophthalmology, pain management, gastroenterology, and orthopedics in 2018 and 2023, and Table 1 shows the percentage change in each SOC’s relative utilization during that period.
Figure 1. Site of Care Breakdown for Select Procedures, Medicare, 2018 and 2023
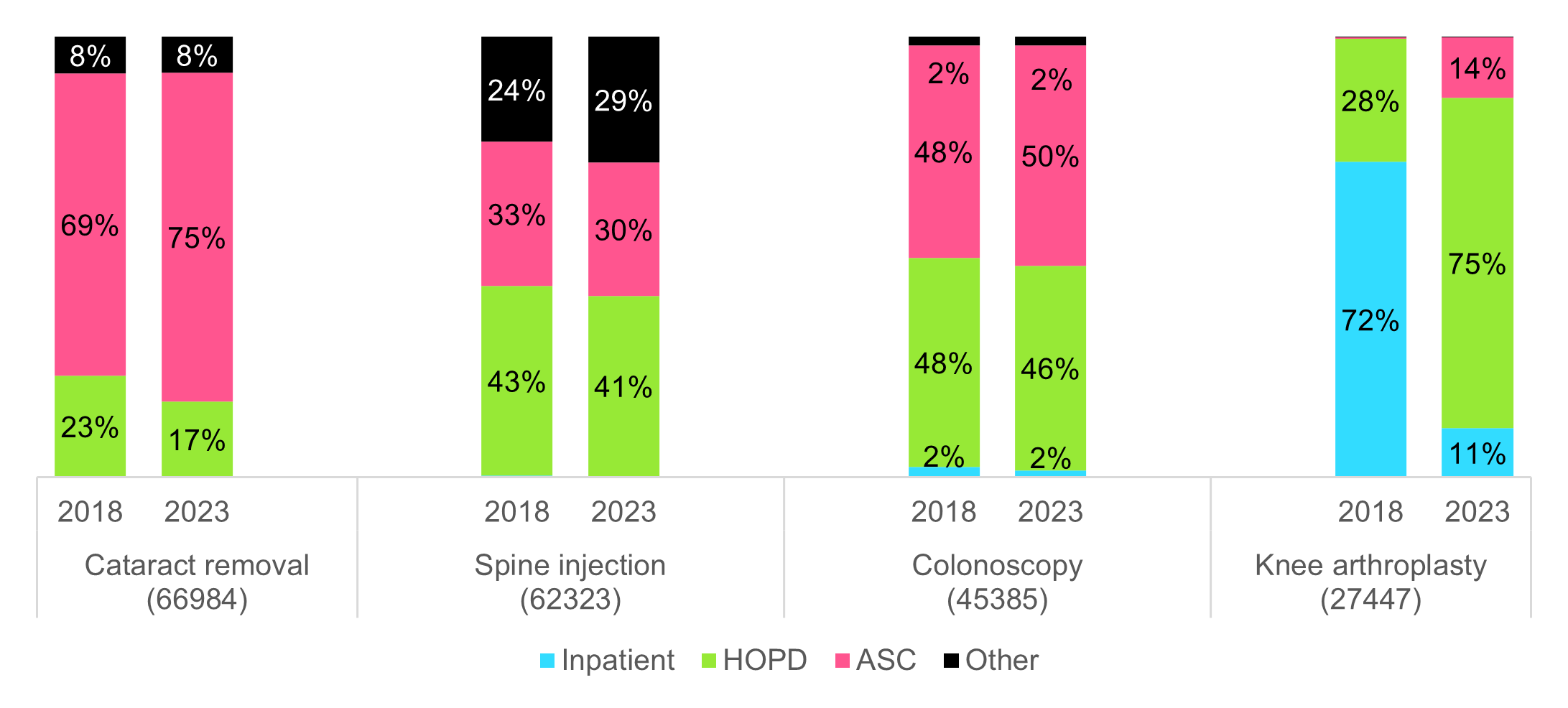
Note: “Other” includes all SOCs other than inpatient, HOPD, and ASC. Volume in this category for the above procedures is generally synonymous with in-office utilization.
Table 1. Shift in Site of Care for Select Procedures, Medicare, 2018 to 2023
| Inpatient | HOPD | ASC | Other | Total 2023 Utilization | |
|---|---|---|---|---|---|
| Cataract removal (66984) | 0% | -6% | +6% | -0% | 3,162,537 |
| Spine injection (62323) | 0% | -2% | -2% | +5% | 813,895 |
| Colonoscopy (45385) | -1% | -1% | +2% | 0% | 1,964,356 |
| Knee arthroplasty (27447) | -61% | +47% | +13% | 0% | 776,499 |
Note: Some percentage changes may not sum perfectly due to rounding. Source: 100% Medicare Fee-for-Service file, 2018-2023
Using the 100% Medicare data file, Avalere Health’s analysis of these representative codes suggests four different paradigms of SOC shift, each with its own implications for SOC optimization (Table 2)
Table 2. Site-of-Care Optimization Paradigms
| Procedure Archetype | Current SOC Dynamics | Recent Shifts | Future Directions |
|---|---|---|---|
| Cataract removal (66984) | • Can be performed in any outpatient setting • No inpatient volume |
• Modest migration of utilization from the HOPD to the ASC • Stable minority of utilization in the office |
• Likely continued shift from the HOPD to the ASC, gradually increasing the relative dominance of the ASC |
| Spine injection (62323) | • Can be performed in any outpatient setting • No inpatient volume |
• Utilization more evenly spread between the HOPD, the ASC, and the office • Over time, shifts away from the HOPD and the ASC to the office |
• Ongoing clinical and administrative developments (e.g., availability of image guidance in lower-acuity SOCs, payer requirements, etc.) may continue shift to the office |
| Colonoscopy (45385) | • Can be performed in the inpatient, HOPD, and ASC settings • Negligible inpatient volume |
• Relatively stable, with minor incremental shift from the HOPD to the ASC | • Likely continued stability, until reimbursement pressure, payer SOC requirements, site-neutral payment policy, or other forces incentivize further SOC shift |
| Knee arthroplasty (27447) | • Can be performed in inpatient, HOPD, and ASC settings • Removed from IPO list January 1, 2018 • Added to ASC CPL January 1, 2020 |
• In 2018 (first year off IPO list), nearly 30% of volume occurred in the HOPD • In 2024, nearly 90% of volume occurred in the HOPD or the ASC |
• Major initial shift away from the inpatient setting achieved • Ongoing potential to shift volume from the HOPD to the ASC |
Note: These paradigms are not exhaustive. They do not address procedures that are on the IPO list and/or have not yet been added to the ASC CPL. A procedure on the IPO list is not eligible for SOC optimization; once it is removed, it typically experiences a “probationary” period of HOPD utilization lasting one to three years, after which it may be added to the ASC CPL. Optimization occurs as volume shifts to the HOPD and/or the ASC.
These paradigms generalize several archetypal paths toward SOC optimization for specialty services. Some procedures may already have more “mature” SOC optimization (i.e., a high proportion of utilization in the lowest-acuity setting), while other procedures may have more “runway” with respect to SOC shift. At a high level, some specialties, such as pain management, have converted a material proportion of utilization to the lowest-acuity SOC; others, such as orthopedics, have done so for some procedures; and still others, such as cardiology, are earlier in this transition.
Importantly, SOC shifts often depend upon changes in CMS or commercial payer policy. In the absence of changes to the IPO or the ASC CPL, which commercial payers typically follow, SOC patterns can stagnate. For example, Avalere analysis of 100% Medicare data showed that, from 2017 to 2022, there were no major changes to SOC policies for key otolaryngology (ear, nose, and throat) procedures. As a result, the changes in SOC utilization during this period were minimal (typically less than a 3% shift) and directionally mixed (some procedures shifting to the HOPD and others to the ASC or office)
While the SOC for specialty services has long-term relevance to clinical quality and physician practice dynamics, the most immediate impact is to cost. Figure 2 shows the difference in cost between the HOPD and the ASC for CPT code 45385 (colonoscopy), and Table 3 shows the implied savings if all instances of the selected procedures performed in the HOPD were instead performed in the ASC. The HOPD and the ASC have the same professional fee in Medicare, so the difference in procedure price is 100% attributable to difference in facility fee.
Figure 2. Total Medicare Procedure Price for CPT Code 45385 (Colonoscopy), 2025
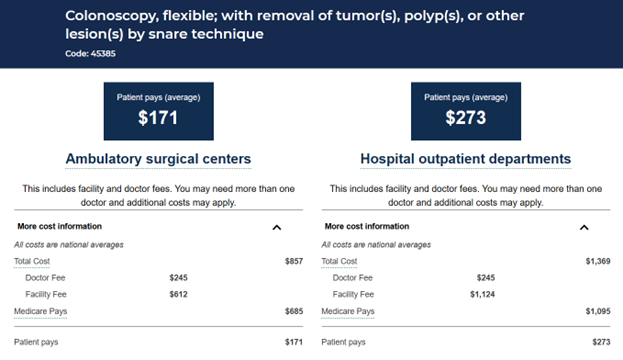
Source: Medicare Procedure Price Lookup Tool
Table 3. Implied Savings from HOPD-to-ASC Shift for Selected Procedures, 2023
| Total HOPD Price | Total ASC Price | Total Price Difference | HOPD Volume | Implied Savings | |
|---|---|---|---|---|---|
| Cataract removal (66984) | $2,701 | $1,643 | $1,058 | 543,607 | $575.3M |
| Spine injection (62323) | $743 | $434 | $309 | 333,217 | $102.9M |
| Colonoscopy (45385) | $1,335 | $816 | $519 | 912,926 | $473.9M |
| Knee arthroplasty (27447) | $14,348 | $10,622 | $3,726 | 583,526 | $2,174.1M |
Source: 100% Medicare Fee-for-Service File, 2023; Hospital Outpatient Prospective Payment and ASC Final Rule Addenda, 2023
Conclusion
While each individual patient’s acuity and clinical circumstances will continue to determine the most appropriate SOC for any given service or procedure, the opportunity to shift certain types of care in the aggregate toward lower-acuity SOCs represents a meaningful opportunity to address healthcare expenditures. Providers can demonstrate value to patients and payers by rendering services in lower-acuity, lower-cost SOCs, and evolving clinical standards and payment policies (e.g., site-neutral payment) will simultaneously shape SOC optimization.
If your organization would like to discuss site-of-care, specialty services, or physician practice management, connect with us.
Related Content



Services
From beginning to end, our team synergy
produces measurable results. Let's work together.
produces measurable results. Let's work together.


