Chronic Care Management in Medicare: Optimizing Utilization
Summary
CCM services remain underutilized, but a subset of claims lacking supporting diagnoses suggests opportunities to improve utilization via coding accuracy.Background
Chronic care management (CCM) is considered an essential primary care service aimed at improving patient care and health outcomes. CCM, which can be provided by providers or their clinical staff, encompasses a range of non-patient-facing services, such as facilitating preventive care, supporting health goals, managing care transitions, and sharing patient health information within and across care teams. Evidence suggests that CCM in Medicare can improve care: a federally funded study found that CCM improves clinician efficiency, patient satisfaction, therapy adherence, and reduces hospitalizations and emergency department (ED) visits, resulting in savings of $74 per member per month, or $888 annually per beneficiary.
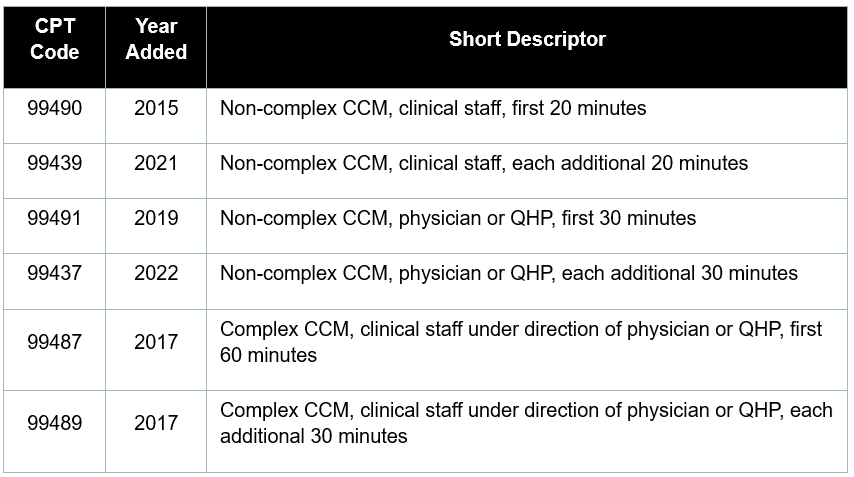
Relevant Services: The Centers for Medicare and Medicaid Services (CMS) pays for CCM services for eligible patients under six relevant codes: 99437, 99439, 99487, 99489, 99490, and 99491 (Appendix). CMS has also introduced several other code families to support similar, and sometimes mutually exclusive, coordinated care services, including transitional care management, advanced primary care management, principal care management, and CCM specifically for pain management.
Eligible Patients: To qualify for CCM, patients must have at least two chronic conditions expected to either persist for at least 12 months or pose a significant risk of death, acute exacerbation, decompensation, or functional decline. Examples of qualifying chronic conditions include diabetes, hypertension, chronic kidney disease, heart failure, cancer, arthritis, and Alzheimer’s disease. In addition to the number of underlying conditions, CMS suggests that practitioners also consider the number of medications, repeat admissions, and past ED visits when identifying patients who are eligible for CCM.
Analysis
Amid growing interest in CCM and incentives for its use, Avalere Health analyzed CCM utilization trends in Medicare claims from 2019 to 2023. To understand the extent of utilization growth, we determined the number of Medicare beneficiaries who received CCM services, the total number of CCM claims submitted, and the average number of claims per beneficiary. Because CCM is intended for beneficiaries with two or more chronic conditions, we also analyzed the distribution of chronic conditions among those who received CCM services. Further methodology information is included in the Appendix.
Results
CCM Uptake: Two-thirds of Medicare beneficiaries have two or more chronic conditions and many are likely eligible to receive CCM services. However, only a fraction of eligible beneficiaries have been enrolled in a CCM program. At least one study suggested that initial uptake was low, with less than 4% of eligible enrollees receiving CCM care in 2019.
Recognizing the potential of CCM to enhance both patient outcomes and cost efficiency, CMS has taken meaningful steps to expand the program by introducing new CPT codes for additional service time and raising reimbursement rates by increasing the underlying work relative value units (RVUs) in 2022 (Figure 1). The largest increases (81% to 100%) were observed in the complex CCM codes.
Figure 1. Updates to Work RVUs, 2022
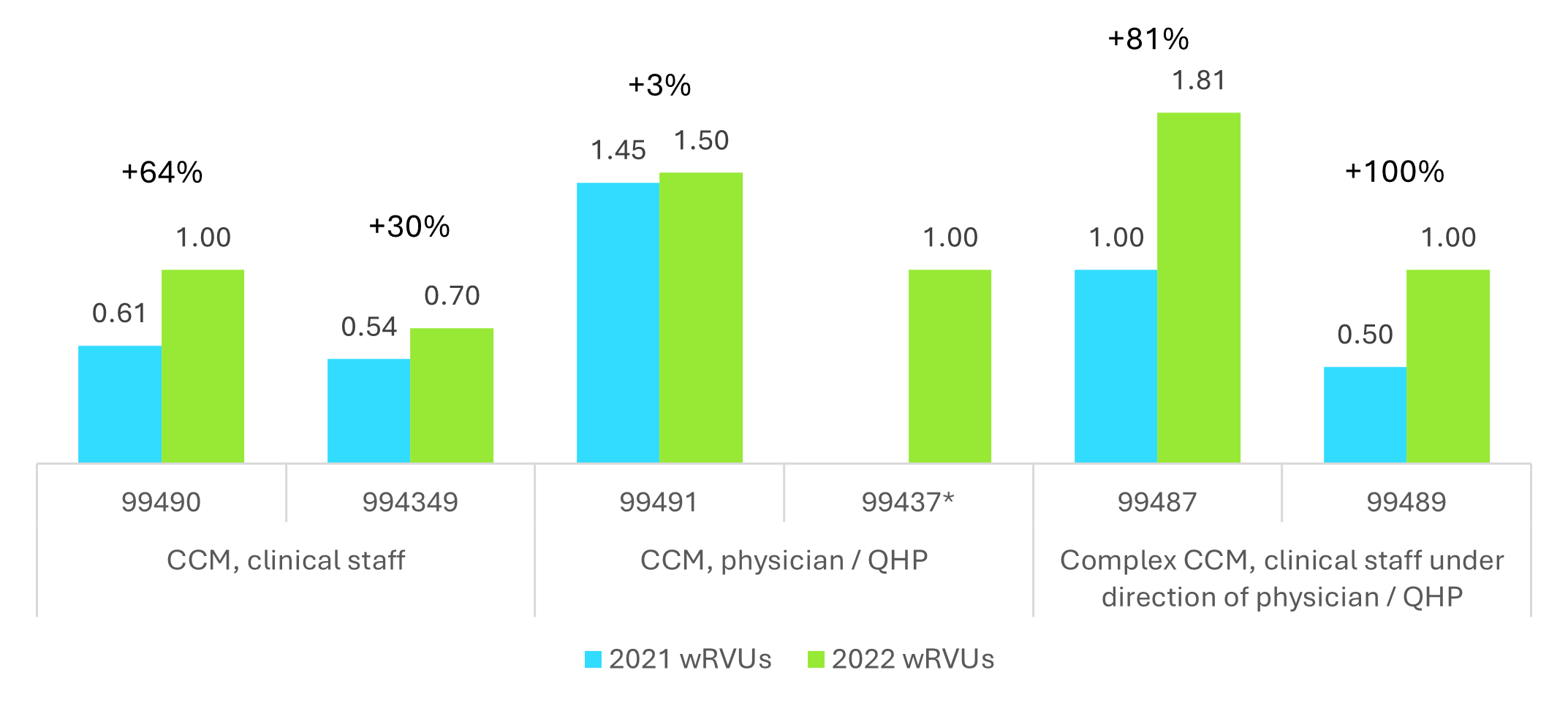
QHP: Qualified Healthcare Professional. Note: CPT code 99437 was new in 2022.
As a result of policy changes intended to more accurately value these services, utilization of CCM codes has increased steadily over the past five years, seeing an average annual growth rate of 7.4% from 2019 to 2023 (Table 1). The largest year-over-year increase was observed after the code set was revalued: the number of Medicare beneficiaries receiving any CCM service increased by 23.4% between 2022 and 2023, when nearly 1.3 million Medicare beneficiaries received CCM.
Table 1. Trends in CCM Utilization, 2019-2023
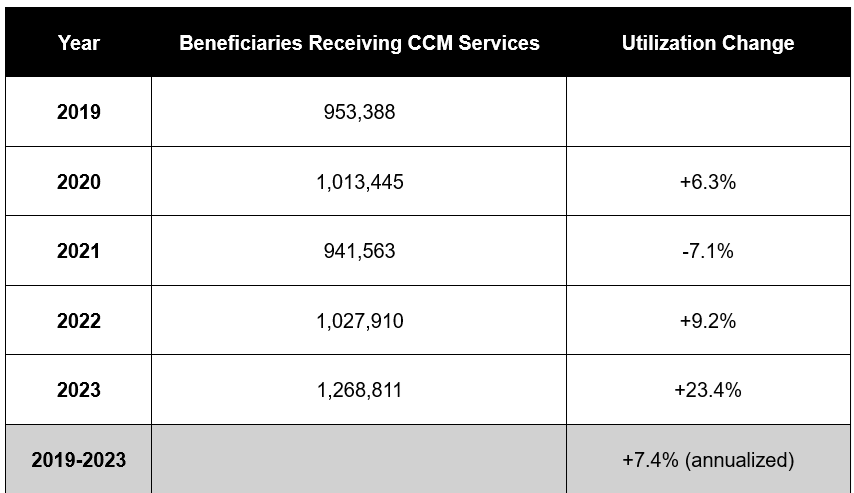
Source: Medicare 100% fee-for-service data
While implementation of CCM has led to increased utilization, our analysis found that—despite growth in beneficiary participation and total claims—opportunities remain to further expand the uptake of CCM services.
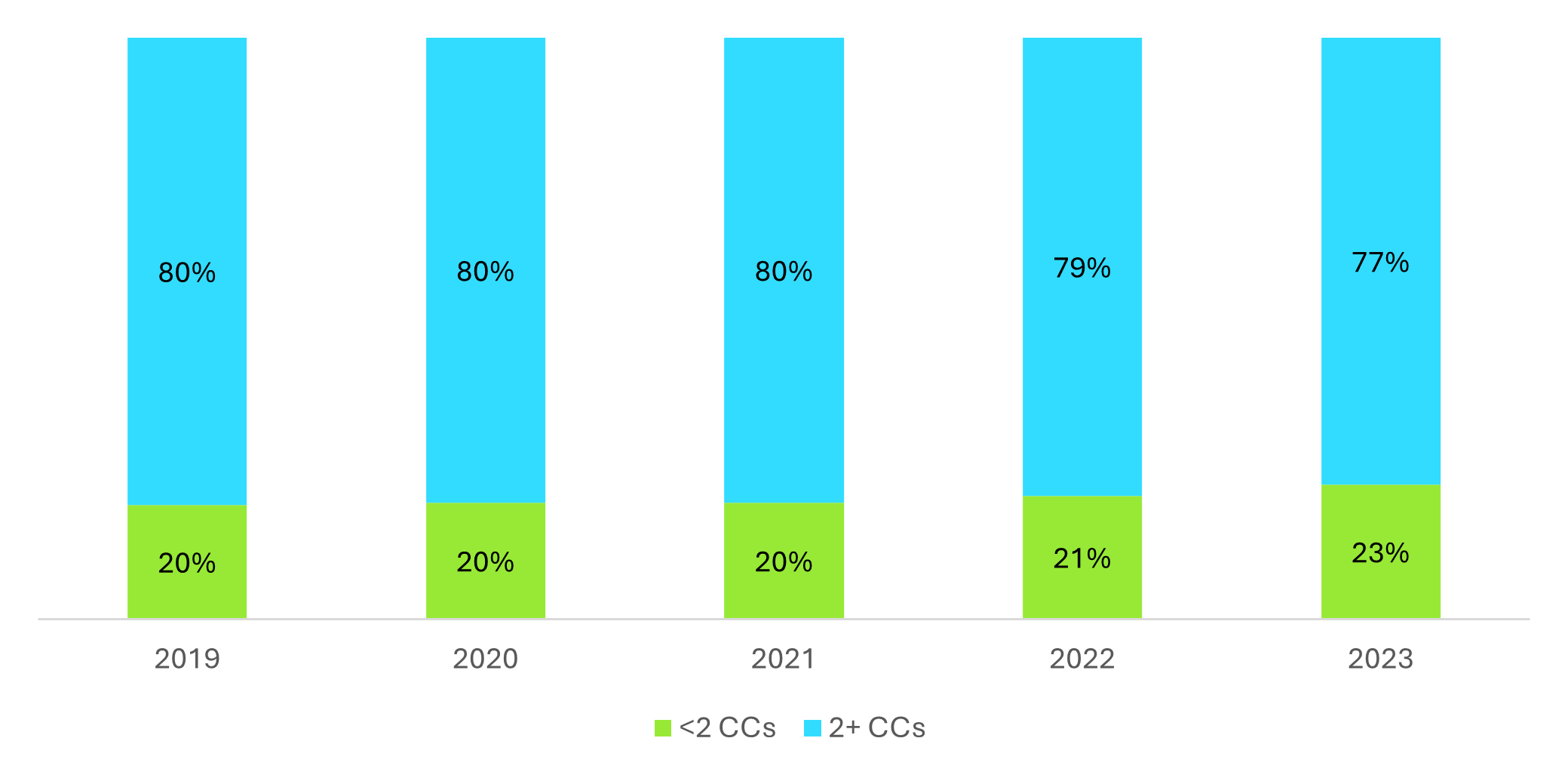
Gap Analysis: CCM may be underutilized among eligible beneficiaries, but not all current recipients of CCM services appear to meet the eligibility requirement of having two or more chronic conditions. According to Avalere Health’s analysis, in 2023 only 77% of billed CCM services were for patients with two or more chronic conditions recorded on the claim; in contrast, 18% of beneficiaries had only one chronic condition recorded, and 5% had none (Figure 2). Given that the portion of claims lacking sufficient documentation increased as CCM utilization increased, these anomalies raise questions about coding accuracy and the consistency of eligibility assessments.
Figure 2: CCM Claims by Number of Chronic Conditions Reported, 2019–2023
 Drivers of Low CCM Uptake
Drivers of Low CCM Uptake
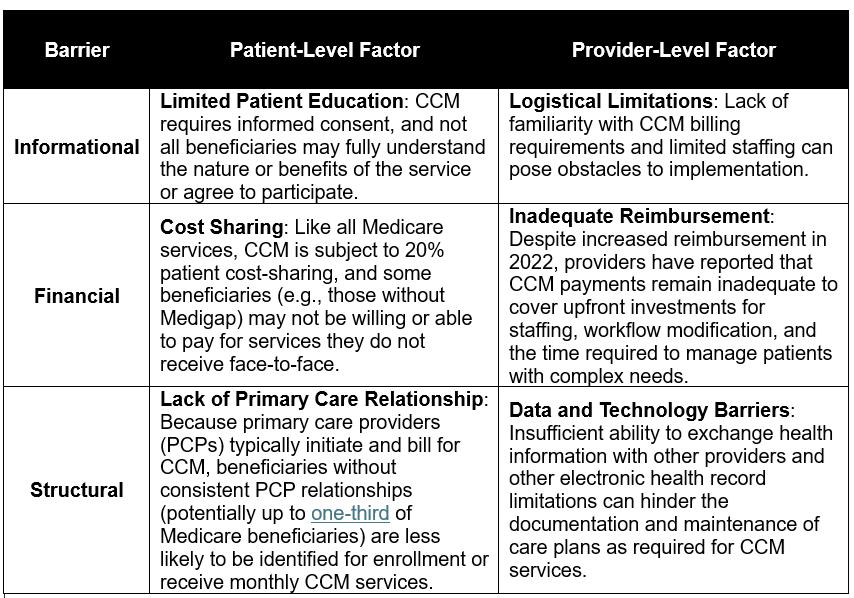
While utilization of CCM services has increased over time, the breadth and consistency of their uptake remains uneven. This limited adoption is likely influenced by a combination of patient- and provider-level factors.
Table 2. Barriers to Appropriate CCM Uptake
Some providers have suggested that CMS could play a greater role in educating beneficiaries about CCM’s value to help facilitate consent and engagement. Our claims analysis suggests two key areas for improvement among providers: proper documentation of diagnoses and improved consistency of CCM utilization. We did not assess the clinical appropriateness of the services billed.
Opportunities for Improvement
While the underlying cause of the discrepancy in diagnosis coding on CCM claims is unknown, it could reflect a lack of financial or operational incentives for precise diagnosis coding within traditional Medicare. Though providers serving both traditional Medicare and Medicare Advantage (MA) beneficiaries can deliver CCM services, the risk-adjusted payments in MA reward create incentives to report diagnoses completely and accurately. In contrast, traditional Medicare reimburses providers on a fee-for-service basis with no diagnosis-based adjustment, potentially contributing to less accurate coding practices.
Additionally, the Medicare claims data show evidence of inconsistent service provision. In 2023, 6.5 million CCM claims were submitted; this is an average of 5.1 per beneficiary and a slight increase from the average of 4.9 claims per beneficiary in 2019. Since providers can bill monthly for CCM services and CMS expects that the full scope of services be delivered each month (unless not medically necessary), this lower-than-expected frequency suggests barriers to consistent care coordination that have persisted over time.
Looking Ahead
Further exploration is needed to fully understand the patterns of CCM uptake and service provision. Insights from this analysis can inform strategies that support broader participation in CCM programs to improve patient care and contribute to Medicare cost savings.
To learn more about CCM and other trends in primary care, connect with us.
Appendix: CCM Code Descriptions and Methodology
Related Content


Services
From beginning to end, our team synergy
produces measurable results. Let's work together.
produces measurable results. Let's work together.


